
Comparison of SERVE-HF and ADVENT-HF Trials
| Aspect | SERVE-HF Trial | ADVENT-HF Trial |
|---|---|---|
| Population Studied | Heart failure patients with reduced ejection fraction (HFrEF) and predominant central sleep apnea (CSA). | Heart failure patients with sleep apnea (central and obstructive sleep apnea [OSA]). |
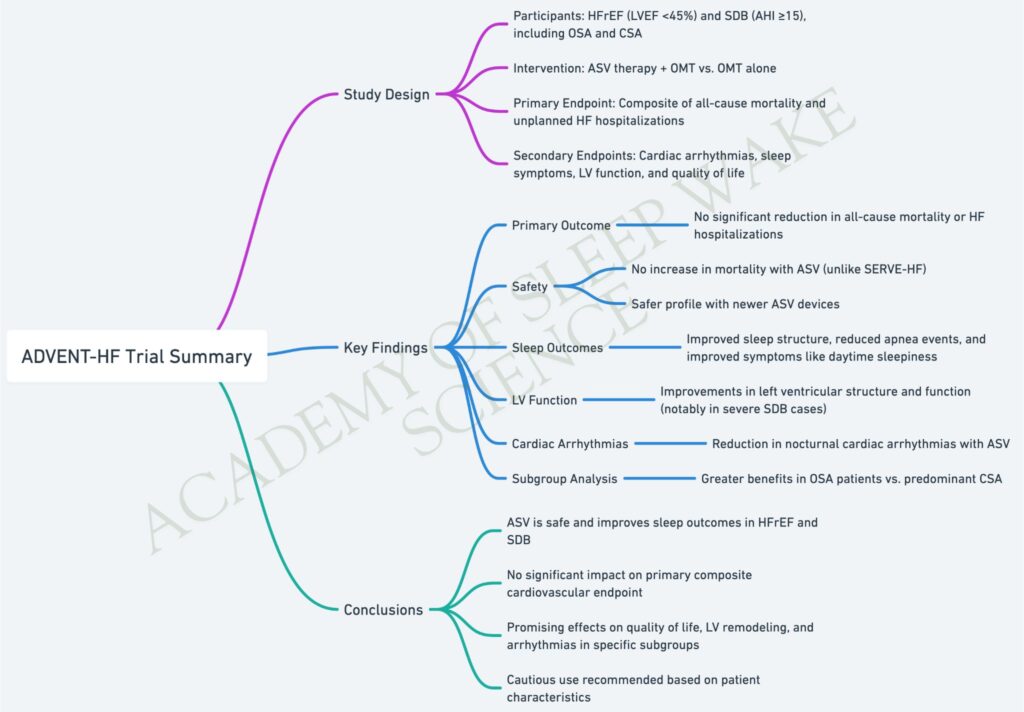
| Primary Objective | Evaluate the impact of Adaptive Servo-Ventilation (ASV) on mortality and morbidity in HFrEF patients with CSA. | Assess the safety and efficacy of ASV in reducing cardiovascular events and improving QoL in heart failure. |
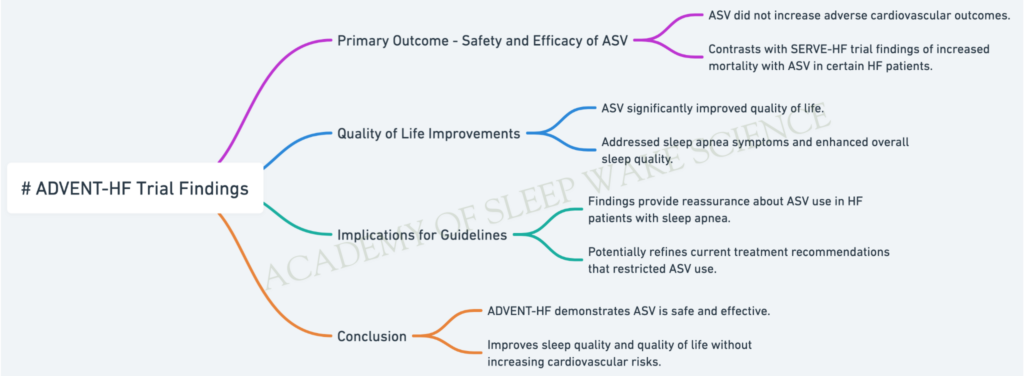
| Primary Findings | – ASV increased cardiovascular mortality, particularly in patients with severely reduced LVEF (≤30%). | – ASV did not increase cardiovascular risk, contrasting with SERVE-HF findings. |
| – ASV did not reduce the primary composite endpoint (all-cause death or hospitalization for heart failure). | – ASV improved sleep quality and symptoms but did not significantly reduce major cardiovascular events. | |
| Cardiovascular Mortality | ASV was associated with a higher cardiovascular mortality (HR: 1.34). | ASV did not increase cardiovascular mortality, showing a neutral effect. |
| Quality of Life (QoL) | No significant improvement in QoL despite using ASV. | ASV significantly improved QoL and reduced sleep apnea-related symptoms (e.g., daytime sleepiness). |
| Impact on Sleep Apnea | ASV effectively reduced central apneas but had no significant benefit on overall outcomes. | ASV improved both central and obstructive sleep apnea indices, enhancing sleep-related outcomes. |
| Key Mechanistic Insight | Sudden cardiac death and arrhythmias were hypothesized as the cause of increased mortality with ASV. | Showed that ASV can be safely used in patients without increasing cardiovascular risks. |
| Study Limitations | – Excluded patients with OSA, limiting generalizability. | – Broader inclusion criteria but fewer specific subgroup analyses. |
| Adverse Effects | Increased cardiovascular mortality in patients with severe HFrEF. | No evidence of increased adverse cardiovascular outcomes. |
| Clinical Implication | ASV is contraindicated in HFrEF patients with CSA and LVEF ≤45%. | ASV is safe and improves QoL in heart failure patients with sleep apnea, but cardiovascular benefits remain unclear. |
| Conclusion | ASV is harmful in HFrEF with CSA and should not be used in this population. | ASV is safe and effective in improving symptoms and QoL, with no increase in cardiovascular risk. |
Summary
- SERVE-HF: Found that ASV increased cardiovascular mortality and had no overall benefit in HFrEF patients with CSA, leading to contraindications in this group.
- ADVENT-HF: Demonstrated that ASV is safe and improves symptoms and QoL in heart failure patients with sleep apnea, though it did not significantly reduce major cardiovascular events.
These trials highlight the importance of understanding the differences between central and obstructive sleep apnea in heart failure and tailoring treatment accordingly.